")
")
")








Comment on a new study of the embryotoxicity of various Chinese herbal medicines with unreliable results
Lu Li and a team of scientists from Hong Kong and Germany published a study (1) comparing the alleged embryotoxicity of ten Chinese herbal medicines according to animal tests with the results of new in vitro tests they carried out. The following herbal medicines were tested for the designated characteristics:
- Tripterygii wilfordii Radix (lei gong teng), considered obsolete due to considerable toxicity;
- Hirudo (shui zhi), the leech, traditionally contraindicated during pregnancy;
- Trichosanthis Radix (tian hua fen), traditionally contraindicated during pregnancy;
- Coptidis Rhizoma (huang lian), contraindicated during pregnancy according to modern research (2);
- Astragali Radix (huang qi), with no known risk during pregnancy;
- Paeoniae Radix (bai shao), with no known risk during pregnancy;
- Scutellariae Radix (huang qin), with no known risk during pregnancy;
- Notoginseng Radix (san qi), traditionally used with caution during pregnancy;
- Carthami Flos (hong hua), contraindicated during pregnancy according to modern research (2).
- Salviae miltiorrhizae Radix (dan shen) is traditionally contraindicated during pregnancy due to the risk of miscarriage.
First, these herbal medicines were categorized according to their presumed level of embryotoxicity, as described in the literature: strong, weak, or non-existent. However, these classifications are incorrect in several respects. Tripterygii wilfordii Radix (lei gong teng) and Hirudo (shui zhi) are accurately classified as strongly embryotoxic. However, for Trichosanthis Radix (tian hua fen), which is also classified as strongly embryotoxic, no usable data applicable to a decoction or granules exists. The study by Li et al. presents data on trichosanthin, a protein isolated from Trichosanthis Radix that has a strong abortifacient effect and has been used clinically by injection for this purpose. This application has been discontinued due to frequent allergic reactions. In addition to being abortifacient, trichosanthin displayed embryotoxic and teratogenic effects in animal tests. The protein is probably denatured by heat, which might render it ineffective. Although embryotoxic risk cannot be ruled out, these data cannot be applied to a whole extract of Trichosanthis Radix derived from a decoction. The available data cannot confirm or exclude the embryotoxicity of Trichosanthis Radix.
Similarly, the data on Astragali Radix (huang qi) is inconclusive regarding possible embryotoxicity. So far, animal-testing-based studies only exist relating to the substance astragaloside IV. In rabbits and/or rats, there was an increased number of stillbirths, as well as developmental retardation in some cases, though no malformations were observed (3-6). Based on these data, it is not possible to formulate a statement regarding the whole extract of Astragali Radix.
Coptidis Rhizome (huang lian) is described by Li et al., based on literature data, as "weakly embryotoxic." Chuang et al.'s comparatively minor study (7) shows a slight, non-significant decrease in birth weight of newborns. Yet, a crucial study by the same authors (8) demonstrating a significant risk of malformation when mothers took this medicine during the first trimester of pregnancy is ignored. Therefore, Coptidis Rhizome has to be considered strongly embryotoxic, particularly due to the existence of human data.
Paeoniae Radix Alba (bai shao) is considered to have a low risk of embryotoxicity; however, no literature references are provided. A decoction of the medicine showed no embryotoxic or teratogenic effects in mice, a test on stem cells revealed no significant cytotoxicity (9).
A lack of embryotoxicity for Scutellariae Radix (huang qin), Notoginseng Radix (san qi) and Salviae miltiorrhizae Radix (dan shen) is compatible with the literature. On the other hand, the pronounced embryotoxicity of Carthami Flos (hong hua) was not acknowledged. A decoction or aqueous extract of this medicine showed, as well as a higher rate of miscarriage, an increased rate of stillbirths, delays in fetal development and deformities in rats (10, 11). In mice, there was an increased incidence of embryo death and likewise a higher rate of stillbirths and deformities (12, 13).
Thus much of the information on allegedly known embryotoxicity of the 10 herbal medicines represents either an under- or overestimate; in two cases an evaluation is not possible due to a lack of meaningful data. The study by Li et al. used various in vitro tests for determining the embryotoxicity of these medicines, and compared their results with the (allegedly) known embryotoxicity from in vivo tests. In vitro methods offer the advantage of sparing experimental animals. The question is, how well can they predict embryotoxicity risk and/or to what extent do their results correlate with those of in vivo tests. 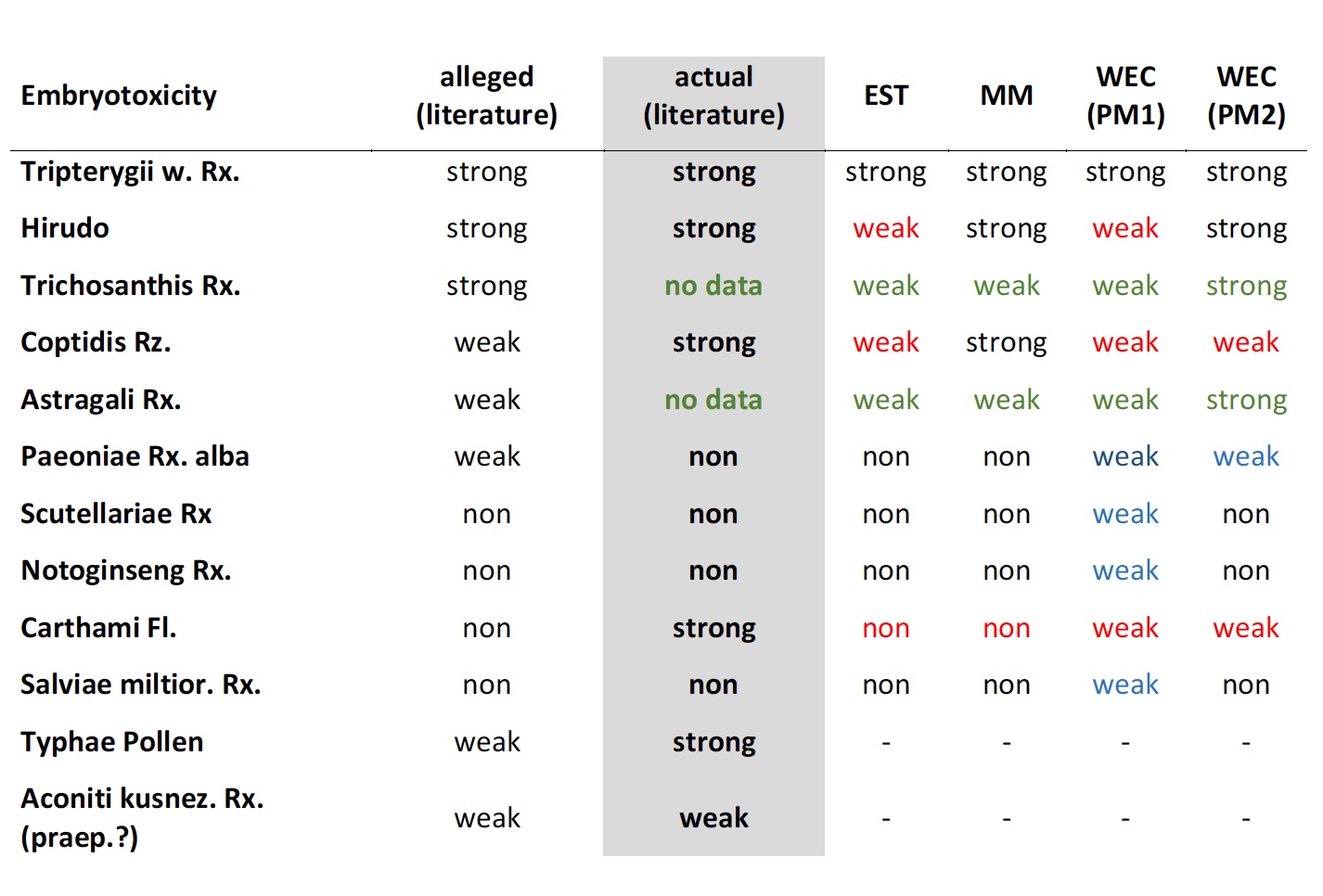 Table: Comparison of in vivo embryotoxicity according to the literature (alleged and actual) with the in vitro results of various test procedures by Li et al. (1).
Table: Comparison of in vivo embryotoxicity according to the literature (alleged and actual) with the in vitro results of various test procedures by Li et al. (1).
The study group applied three different testing systems: the embryonic stem cell test (EST), the micromass (MM) and the whole embryo culture (WEC) in two forms: WEC (PM1) and WEC (PM2). An overview of the alleged and the actual known in vivo embryotoxicity, as well as the embryotoxicity prediction from the various in vitro tests is shown in the table. For the medicines Trichosanthis Radix (tian hua fen) and Astragali Radix (huang qi), no information regarding known embryotoxicity can be given, as no valid data exist. It is evident that many of the in vitro results differ from previously known risk data. The strong embryotoxicity of Hirudo is only identified as such in 2 out of 4 tests, that of Coptidis Rhizoma in only 1 out of 4; the well-documented strong embryotoxicity of Carthami Flos is not detected as such at all. On the other hand, the results of several in vitro tests indicate weak embryotoxicity for medicines to which none had previously been attributed.
Conclusion
The study by Li et al. does not accurately reflect previously known in vivo embryotoxicity. The pronounced embryotoxicity of Coptidis Rhizoma and Carthami Flos is underestimated or negated. The alleged weak embryotoxicity of Paeoniae Radix Alba is not substantiated and contradicts data from the literature. Numerous errors in citations, quoted numerical data, and units that differ from the literature will not be addressed in detail here. The in vitro test procedures presented are an interesting contribution. However, their results for eight herbal medicines bear limited correlation to previously known results from the literature. The extent to which in vitro tests for the reproductive toxicity of Chinese herbal medicines can replace in vivo studies requires further research.
Axel Wiebrecht
References
- Li L, Yin Tang L, Liang B, et al. Evaluation of in vitro embryotoxicity tests for Chinese herbal medicines. Reprod Toxicol. 2019;89:45-53.
- Wiebrecht A. Sicherheit in der Chinesischen Arzneitherapie. In: Focks C, ed. Leitfaden Chinesische Medizin. 7thed. München: Elsevier; 2017:978-1028,1160-1164.
- Zhu JB, Zhu YP, Zhang TG. [Evaluation of toxicity of astragaloside IV in rats and rabbits] (Chinese). Du Lixue Zazhi [Journal of Toxicology]. 2007;21(4):317-318.
- Zhu JB, Wan XY, Zhu YP, et al. Effect of astragaloside IV on the embryo-fetal development of Sprague-Dawley rats and New Zealand White rabbits. J Appl Toxicol. 2009;29(5):381-385.
- Zhu YP, Zhang TB, Wan XY, et al. [Study on the teratogenicity of astragaloside IV in SD rats] (Chinese). Zhong Chengyao [Chinese Traditional Patent Medicine]. 2010;32(10):1783-1785.
- Wan XY, Zhu JB, Zhu YP, et al. Effect of astragaloside IV on the general and peripartum reproductive toxicity in Sprague-Dawley rats. Int J Toxicol. 2010;29(5):505-516.
- Chuang CH, Lai JN, Wang JD, et al. Use of Coptidis Rhizoma and foetal growth: a follow-up study of 9,895 pregnancies. Pharmacoepidemiol Drug Saf. 2006;15(3):185-192.
- Chuang CH, Doyle P, Wang JD, et al. Herbal medicines used during the first trimester and major congenital malformations: an analysis of data from a pregnancy cohort study. Drug Saf. 2006;29(6):537-48.
- Xu W, Xu L, Deng B, et al. The potential impact of Radix Paeoniae alba in embryonic development of mice. Phytother Res. 2017;31(9):1376-1383.
- Lin BH, Yan DP, Zhou LR, et al. [Toxicity and effects of Flos Carthami on rat pregnancy and embryonic development] (Chinese). Anhui Zhongyi Xueyuan Xuebao [Journal of Anhui University of Chinese Medicine]. 1998;17(4):50-52.
- Zhao YL, Feng B, Zhou Y, Zhang J. [Study on selective expression of toxicity of Flos Carthami in pregnant rats] (Chinese). Liaoning Zhongyi Zazhi [Liaoning Journal of TCM]. 2011;38(11):2274-2276.
- Nobakht M, Fattahi M, Hoormand M, et al. A study on the teratogenic and cytotoxic effects of safflower extract. J Ethnopharmacol. 2000;73(3):453-459.
- Song XQ, Li JH, Wei HP, et al. [Effects of Flos Carthami on estrogen/progesterone and their receptors in early pregnancy of mice] (Chinese). Zhongguo Xiandai Yixue Zazhi [China Journal of Modern Medicine]. 2014;24(32):5-8.
A new study on liver injury caused by Chinese herbal medicines: substantial data, questionable conclusions
A new study on liver injury caused by Chinese herbal medicines: substantial data, questionable conclusions
Dec, 2017, slightly modified Jun, 2026
The study
A recent study by Melchart and co-authors [1] analysed the incidence of liver injuries occurring in an TCM hospital in Kötzting, Germany from 1994 to 2015. Included were patients treated with Chinese herbal therapy whose liver enzyme ALT (alanine aminotransferase) at the time of admission was within the normal range. Just before discharge, the liver function was checked again. An elevation of ALT up to 5 times the upper norm was considered as an adaptive phenomenon of the liver, and a higher increase was interpreted as liver injury. The average treatment time was 19.5 days due to the duration of inpatient stay. The association of liver injury with the Chinese medicines was assessed using the internationally accepted RUCAM (or CIOMS) scale [7].
21,740 patient cases were evaluated. An ALT elevation above the normal range was observed in 3.93% of cases, and liver injury with an at least 5-fold ALT elevation occurred in 26 patients (0.12%). In 8 out of these 26 patients, the authors stated a "probable" association with Chinese herbs, in 16 cases a "possible" association, and in 2 cases they excluded a causality. Bupleuri Radix (chai hu) and Scutellariae Radix (huang qin) particularly stand out, as they were involved in 7 of the "probable" or "possible" cases, in 6 of which both were involved simultaneously.
In their analysis, the authors supposed a known hepatotoxicity for a number of herbs („associated with potential liver injury as evidenced from the scientific literature“) which were involved in the cases, namely Bombyx batryticatus (jiang can), Dictamni cortex (bai xian pi), Ephedrae herba (ma huang), Glycyrrhizae radix (gan cao), Polygoni multiflori caulis (shou wu teng), Polygoni multiflori radix (he shou wu), Polygoni cuspidati rhizoma (hu zhang), Psoraleae fructus (bu gu zhi), Puerariae radix (ge gen), Rhei radix et rhizoma (da huang), Sennae folium* (fan xie ye) and Toosendan fructus* (chuan lian zi).
*Name has been adjusted to the current nomenclature.
Commentary
This study provides valuable, unprecedented data for assessing the potential risk of Chinese herb-induced liver injury, characterised by the following features:
- the prospective design
- the high number of 21,470 included patients which allows a valid estimate of the incidence of liver injuries in non-predisposed patients within a limited period of time (19.5 days on average)
- the prior authentication and testing for contamination of the herbs used
- reference to European conditions by exclusion of prohibited substances, the most toxic medicinals which are uncommon in this area, and the use of excessively high doses
- and last but not least, full transparency regarding all components of the herbal formulas and the calculation of the RUCAM scores.
This is thanks to the authors. An important signal is that relevant liver injury caused by Chinese herbs - at least under the conditions of the study - rarely occurs, and after the discontinuation of therapy, usually regresses uneventfully. However, with regard to the interpretation of the results, some comments and corrections to the study appear to be appropriate.
In evaluating the causality between certain herbs and an observed liver injury, the extent to which hepatotoxicity is already considered proven for these herbs is a key point. Known hepatotoxicity leads to an increase of 1 to 2 points in the probability of a causality concerning the RUCAM score used in the study. These points often make the difference between a "possible" and a "probable" association or if one herb or another is suspected of being the causative agent. If an assumption is made without sufficient evidence, one runs the risk of confirming prejudices and reproducing misconceptions. Frequent repetitions do not make statements more true. In addition, evidence of causality assignment can only rely on "probable" or "very probable" associations to avoid misjudgements. "Possible" associations may have a supportive role or may draw attention to certain herbs, but they can not establish evidence.
For several herbs, which were suspected of being hepatotoxic in the study, these reservations are relevant. The most striking example is Glycyrrhizae radix. This is the herb most commonly used in Chinese medicine which is contained in approximately 50% of herbal formulas. If a formula is suspected of liver toxicity, then Glycyrrhizae radix is automatically involved in about half of the cases. The same also applies to other herbs commonly used in Chinese medicine such as Atractylodis macrocephalae rhizoma or Angelica sinensis radix. Therefore, the suspicion is justified only if the involvement of a herb in liver injury is significantly higher than its average frequency of use. Reservation should be used when a particular herb is involved that commonly is prescribed together with a potentially hepatotoxic agent, because both substances are indicated for certain diseases or their effects complement each other. Here, the frequent involvement of a herb can create a wrong picture.
In a previous smaller study from the Kötzting hospital [2], Glycyrrhizae radix and Atractylodis macrocephalae rhizoma stood out significantly as ingredients of herbal formulas associated with liver enzyme elevations. The authors had described these results as possibly due to chance or to confounding factors, since these herbs had not previously been reported as hepatotoxic in the literature. In the current study, Glycyrrhizae radix and Atractylodis macrocephalae rhizoma are involved in only 2 out of 9 cases as being "probably" associated with liver injury, whereupon the inclusion criterion is not based on a 2-fold, but on a more than 5-fold elevation of ALT above upper norm. Nevertheless, a suspected hepatotoxicity for Glycyrrhizae radix in the present study is stated because this property is assumed as being established.
One contributing author repeatedly stressed a hepatotoxicity of Glycyrrhizae radix (gan cao) as having been documented in the literature [3-5] which increased the likelihood of it being associated with liver injury in the present study according to the RUCAM test by 2 points. This assessment is based on two poorly documented case reports within a single publication from Hong Kong [6]. One of these two case reports is sufficient for Teschke and co-authors [3, 5] to establish the hepatotoxicity of three herbs simultaneously, which is hard to reconcile with the laws of logic. The rationale was that the hepatotoxicity of the herbs should be apparently known, but references are not provided by either the authors of the case reports or by Teschke et al. A complete account of the ingredients used in the herbal formulas was missing, as well as the authentication of the herbs or testing for contaminants. The accepted and widely used procedure for assessing the causality of drug-related liver injury is the RUCAM (or CIOMS) test [7]. The scores cited by Teschke et al. [3] for the RUCAM tests are fictitious; the tests were not performed properly. A recalculation resulted in a RUCAM score of 2 or 3 instead of "6 to 8" for the herbs in question, so that the causality is "unlikely" or even "possible" [8]. Thus, these case reports are not appropriate for establishing hepatotoxicity. There is no evidence of hepatotoxicity relating to Glycyrrhizae radix.
Another case is Bombyx batryticatus. Here too, without legitimacy, the authors claim hepatotoxicity as being known. In many larger case compilations of liver injury, this medicine is missing [9-19]. In the publication by B. Shaw [20], Bombyx batryticatus was present, as an ingredient of the complex formulas, in just 2 out of 40 patients with a liver reaction likely or possibly related to Chinese herbal medicine, without it being cause for suggesting a suspected hepatotoxicity. The review by Tu et al. [21] gives a detailed report on the side effects of Bombyx batryticatus, with no mention of liver toxicity. If you search for "Bombyx" and "(liver injury or hepatotoxicity)" in Pub Med, you will find 3 publications that describe a hepatoprotective property of this herb. The work by Teschke et al. [22], which in turn relies merely on the unsuitable Hong Kong case study [6], stands alone in asserting a potential hepatotoxicity.
For a valid causality assessment, clear evidence for the assumption of a "known" hepatotoxicity is required. Herbal medicines, especially those from TCM, involve a particular challenge: they are rarely used as single herbs. In multicomponent herbal formulas, it is difficult to blame a particular ingredient for the reaction. The identity of the herbs must be ensured, since mistakes or deliberate adulterations do occur. Furthermore, contamination due to impurities, undesirable substances or conventional drugs must be excluded. The way in which a herb is prepared or pre-treated, which is often done just to reduce toxicity, can also play a crucial role [9]. Therefore, one cannot unconditionally apply study results from another therapeutic system (e.g., Kampo, Ayurveda) which uses a different method of preparation, to TCM.
The conditions for evidence are fulfilled by only a few herbs. For Polygoni multiflori radix (he shou wu), they are beyond doubt. It is often used as a single herb, too. Among the numerous case reports, authentication or testing for contaminants was partially carried out. For Dictamni cortex (bai xian pi), there are only a few cases of it being used as a single herb [23, 24]. However, it is striking that this herb is significantly more probable to be involved in liver injury than its frequency of use accounts for.
Other herbs with insufficiently documented evidence, which are considered potentially hepatotoxic in the study, are: Sennae folium, Polygoni cuspidati rhizoma, Polygoni multiflori caulis, Pueraria radix and Rhei radix et rhizoma. For example, with Puerariae radix: Teschke et al. [22] cited a reference dealing with two cases of hepatitis due to the juice of Puerariae lobatae radix from Korea [25]. An authentication of the preparations was not documented. The phytochemical composition of the juice cannot be equated with that of a decoction from the dried root as it is used in the context of Chinese medicine. The RUCAM tests which were carried out, each with a high score of 10 [25], are not credible since the differential diagnosis is incomplete and the documentation of the quo ante hepatotoxicity is not sufficiently substantiated.
The updated RUCAM test assigns two points for hepatotoxicity if it is listed in the product characteristic, and one point if there is only evidence in the literature [7]. A product characteristic is missing for raw herbs. TCM finished products with a single herb as the active ingredient exist only as an exception. For the assured, albeit very rare, hepatotoxicity of Polygoni multiflori radix (he shou wu), 2 points can be applied analogously. For other herbs that are mentioned in publications, but for which there is no clear evidence, a rating with a quo-ante score of "1" is appropriate: this applies for Ephedrae herba, Toosendan fructus, Bupleuri radix and Scutellariae radix. For the remaining herbs mentioned in the study, no valid references have been documented which would justify one point.
In several cases, this approach leads to an amendment of the RUCAM assessment (Table 1). Of the 9 study cases whose association with Chinese medicine should be "probable", only 4 remain: cases 3, 12, 14 and 19.2; each with a RUCAM score of 6. This "probable" association applies to the entire herbal formula and can only be applied to a single herb if not more than one ingredient of the formula is suspected of being hepatotoxic. This is true for case no. 12, where only Toosendan fructus with a score of "1" justifies a RUCAM score of 6 for a "probable" association. The RUCAM test states that if other substances are eligible as an alternative cause, "2" points should be deducted [7]. If 2 or more herbs with a pre-existing suspicion of hepatotoxicity are involved, then, if you want to break down the causality to the individual herbs, these 2 points should be subtracted. Then, a "probable" causality can no longer be assumed for these single herbs.
| Fall Nr. | 3 | 4 | 12 | 14 | 17 | 18 | 19(1) | 19(2) | 24 |
|---|---|---|---|---|---|---|---|---|---|
| RUCAM lt. Melchart et al. | 7 | 6 | 7 | 7 | 6? | 6 | 6 | 7 | 6? |
| Zeit bis zur Reaktion | 2 | 2 | 2 | 2 | 2 | 2? | 1→2 | 1→2 | 2 |
| Rückgang der ALT | 2 | 2 | 2 | 3 | 3→2 | 2→0 | 1→3 | 1→3 | 2 |
| Alkoholkonsum | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Alter >55 | 1 | 1 | 1 | 1 | |||||
| Begleitdrogen/-arzneimittel | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| alternative Ursachen | 0→-2 | 0→-2 | 0→-2 | 0 | 0 | 0 | 1→-2 | 1→-2 | -2 |
| vorliegende Inform. ü. Hepatotoxizität | 2→1 | 2→1 | 2→1 | 2→1 | 2→1 | 2→1 | 2→1 | 2→1 | 2→1 |
| Reexposition | 1 | ||||||||
| RUCAM revidiert | 4 | 3 | 4 | 6 | 5 | 3 | 5 | 6 | 3 |
| beteiligte Drogen | |||||||||
| Bupleuri rd. (chai hu) | x | x | x | x | x | x | x | ||
| Scutellariae rd. (huang qin) | x | x | x | x | x | x | x | ||
| Ephedrae hb. (ma huang) | x | x | |||||||
| Toosendan fr. (chuan lian zi) | x | x |
Tab. 1: RUCAM scores and their composition acc. to Melchart et al. (black) and revisions based on the reevaluation (red). In Case 19(2), the patient was re-exposed to certain medicines after 3 years. The scores refer to the decoction as a whole; to assess the individual medicines, the probability score must be reduced by 1 point in each case. Interpretation of the RUCAM score: >8 points: “very likely”, 6–8 points: “likely”, 3–5 points: “possible”, <3 points: unlikely, excluded, or cannot be assessed.
Bupleuri radix and Scutellariae baicalensis Radix deserve special consideration. There is an abundance of cases of hepatotoxicity in Kampo medicine for formulas containing these substances. Mostly often, both herbs are used simultaneously, e.g. in the formula sho-saiko-to (corresponding to xiao chai hu tang). In Chinese medicine, however, liver injury due to these herbs is scarcely known [26]. Kampo herbs are not simply comparable to those of Chinese medicine. For Bupleuri radix, the species Bupleurum falcatum is used in Kampo medicine [27]. In Chinese medicine, the species B. chinense or B. scorzonerifolium are officinal [28]. In Japan, standard formulas are predominantly used as granules. Alcohol can also be part of the extraction solvent [27], which means that the composition of the extracts is not comparable to that of decoctions from Chinese medicine. As to acute toxicity testing, an ethanol extract was more toxic to the liver than an aqueous extract [29].
Within Chinese medicine, there have been only sporadic case reports with inadequate causality criteria [30, 31] in which these herbs appeared. For the first time, the present study documents several cases with formulas containing Bupleuri radix and Scutellariae radix associated with liver injury, where testing for identity and contamination was done. In the 4 cases remaining as "probable" after revision, Bupleuri radix is involved twice and Scutellariae radix three times. In case 3, where both herbs are involved, Ephedrae herba appears as an alternative causative agent, and in case 14 (without Bupleuri radix), the potential causative agent Toosendan fructus is present. A clear assignment to Bupleuri radix or Scutellariae radix is therefore not possible so far. In case 19.2, only these two herbs are present with a potential quo-ante suspicion. Of particular importance here is the patient's rechallenge by a formula which again contained both of these herbs, but only 3 other herbs (Curcumae longae rhizoma, Curcumae radix and Mori ramulus), which were given in the first formula and for which no reasonable suspicion exists. In addition, it is peculiarly striking how many cases with a “possible” causality these two herbs were involved in.
Based on this new data quality, one has to reassess the hepatotoxicity of Bupleuri radix and Scutellariae radix. Either one herb or the other, or both herbs together, should be considered to be potentially hepatotoxic. However, a definite allocation of causality to one or the other herb does not appear to be feasible without reservation according to the current level of evidence. When using either one of these herbs, one must be prepared for the very rare possibility of an idiosyncratic (unpredictable) reaction.
A re-evaluation also seems appropriate for Toosendan fructus. So far, a possible hepatotoxicity only applied in the case of overdose [32]. Now, the herb is implicated in two out of four cases with a probable association; in case 12, without any other suspected herbs included in the formula. Apparently, hepatotoxicity can also occur in the normal dose range. Unfortunately, dosages are not detailed in this study. However, if there is a dose-dependency, it may be more of an intrinsic hepatotoxicity that could be controlled by limiting the dosage.
For a reassessment of Ephedrae herba, the results of the study are not sufficient. This herb is involved in case 3 in which Bupleuri radix and Scutellariae radix are present, so a clear assignment is not possible. The same applies to case 7 and the first formula in case 19 (19.1), for which the association is merely "possible"; in case 20, Bupleuri radix was used simultaneously. The limited number of hepatotoxicity cases involving Ephedra herba documented in the literature must be weighed against the millions of times the drug was used as a dietary supplement, especially in the years previous to 2004. However, with the cases from the present study, this herb shifts into the upper range of a "possible" hepatotoxicity.
Conclusion
The study contains unprecedented data quality for assessing the hepatotoxic risk of Chinese herbal medicines. However, many of the evaluations made in the publication do not hold up. The potential hepatotoxicity of Bupleuri radix or Scutellariae baicalensis radix, or of a combination of both drugs together in the context of Chinese medicine must be deemed adequately secured although a further differentiation currently is not possible. Toosendan fructus, at standard dosages, also appears to be possibly hepatotoxic even though the dosages were not explicitly reported in the respective cases of the study. The possible liver injury caused by Polygoni multiflori radix has already been confirmed, and the study provides no additional support on this. Toxicity cases involving this herb seem to be less common in Western countries than in Asia.
Overall, liver injuries caused by Chinese herbal medicine are very rare and their prognosis, if recognized early enough, is generally uneventful. For a duration of use longer than 19.5 days, as in the present study, the incidence might be higher than reported here. If liver reactions associated with Chinese herbal medicine occur, it is advisable to carry out a full differential diagnostic procedurefull differential diagnostic procedure to either confirm or disprove the causality, so that the evidence regarding Chinese herbs and their actual hepatotoxic risks increases. This applies not only to the Kötzting hospital, but in every case. The Centre for Safety of Chinese Herbal Medicines, CTCA (Centrum für Therapiesicherheit in der Chinesischen Arzneitherapie) is an appropriate address for dealing with this matter.
Literature:
- Melchart D, Hager S, Albrecht S, Dai J, Weidenhammer W and Teschke R. Herbal Traditional Chinese Medicine and suspected liver injury: A prospective study. World J Hepatol 2017;9:1141-1157
- Melchart D, Linde K, Hager S, et al. Monitoring of liver enzymes in patients treated with traditional Chinese drugs. Complement Ther Med 1999;7:208-216
- Teschke R, Zhang L, Long H, et al. Traditional Chinese Medicine and herbal hepatotoxicity: a tabular compilation of reported cases. Ann Hepatol 2015;14:7-19
- Teschke R, Wolff A, Frenzel C and Schulze J. Review article: herbal hepatotoxicity - an update on traditional Chinese medicine preparations. Aliment Pharmacol Ther 2014;40:32-50
- Teschke R, Larrey D, Melchart D and Danan G. Traditional Chinese Medicine (TCM) and herbal hepatotoxicity: RUCAM and the role of novel diagnostic biomarkers such as MicroRNAs. Medicines 2016;3:18
- Yuen MF, Tam S, Fung J, et al. Traditional Chinese medicine causing hepatotoxicity in patients with chronic hepatitis B infection: a 1-year prospective study. Aliment Pharmacol Ther 2006;24:1179-1186
- Danan G, Teschke R. RUCAM in drug and herb induced liver injury: The update. Int J Mol Sci 2015;17:E14
- 8. Wiebrecht A. Dubious pseudoscience – on the alleged hepatotoxicity of Chinese herbal medicines.Bitte link setzen zu: https://www.ctca.center/de/stellungnahmen/kommentare.html
- Teo DC, Ng PS, Tan SH, et al. Drug-induced liver injury associated with Complementary and Alternative Medicine: a review of adverse event reports in an Asian community from 2009 to 2014. BMC Complement Altern Med 2016;16:192
- Chen YF, Cai HD. [Investigation of liver damage associated with Chinese medicines] (Chinese). Yaowu Buliang Fanying Zazhi 1999;1:27-32
- Li XY, Li CQ, Zhang ZM, et al. [Study on traditional Chinese medicine-induced liver injury: from theory to clinical analysis] (Chinese). Zhuanhua Yixue Zazhi 2015;4:244-249
- Chau TN, Cheung WI, Ngan T, et al. Causality assessment of herb-induced liver injury using multidisciplinary approach and Roussel Uclaf Causality Assessment Method (RUCAM). Clin Toxicol2011;49:34-39
- Lee WJ, Kim HW, Lee HY and Son CG. Systematic review on herb-induced liver injury in Korea. Food Chem Toxicol 2015;84:47-54
- Ma X, Peng JH and Hu YY. Chinese Herbal Medicine-induced Liver Injury. J Clin Transl Hepatol 2014;2:170-175
- 1Peng XL, Li CS and Cui SZ. [Biometrical analysis on liver injury caused by traditional Chinese herbs] (Chinese). Shizhen Guoyi Guoyao 1999;10:392-393
- Pittler MH, Ernst E. Systematic review: hepatotoxic events associated with herbal medicinal products. Aliment Pharmacol Ther 2003;18:451-471
- Zhang P, Ye Y, Yang X and Jiao Y. Systematic review on Chinese herbal medicine induced liver injury. Evid Based Complement Alternat Med 2016;2016:3560812
- Zhao P, Wang C, Liu W and Wang F. Acute liver failure associated with traditional Chinese medicine: report of 30 cases from seven tertiary hospitals in China. Crit Care Med 2014;42:e296-299
- Wang XJ, Xu LP and Wang M. [Hepatotoxicity caused by commonly used Chinese medicinal herbs and compound preparations] (Chinese). Shoudu Yike Daxue Xuebao 2007;28:220-224
- Shaw BJ. Aspects of Chinese herbal medicine with relation to their hepatotoxicity. A thesis submitted to King's College London for the degree of Doctor of Philosophy. School of Biomedical and Health Sciences, King's College London & Royal Botanical Gardens, Kew, 2007
- Tu YD, Yu XP. [The clinical use of Bambusa textilis in lung diseases and its side effects] (Chinese). Shanghai Zhongyiyao Zazhi 2012;46:64-66
- Teschke R. Traditional Chinese Medicine induced liver injury. J Clin Translat Hepatol 2014;2:80-94
- Lee JH, Lee HY, Koh KC, et al. [Drug induced liver disease caused by ingestion of Dictamnus dasycarpus] (Korean). Korean J Gastroenterol 1998;31:251-257
- Jang JS, Seo EG, Han C, et al. [Four cases of toxic liver injury associated with Dictamnus dasycarpus] (Korean). Korean J Hepatol 2008;14:206-212
- Kim SY, Yim HJ, Ahn JH, et al. [Two cases of toxic hepatitis caused by arrowroot juice] (Korean). Korean J Hepatol 2009;15:504-509
- Wu SX, Sun HF, Yang XH, et al. ["Re-evaluation upon suspected event" is an approach for post-marketing clinical study: lessons from adverse drug events related to Bupleuri Radix preparations] (Chinese). Zhongguo Zhongyao Zazhi 2014;39:2983-2988
- Japanese Pharmacopoeia (JP XVI). English Version. 16th ed. Tokyo: Pharmaceutical and Medical Device Regulatory Science Society of Japan, 2012
- Chinese Pharmacopoeia Commission. Pharmacopoeia of the Peoples Republic of China (English version). Vol. I. Beijing, China: China Medical Science Press, 2015
- Liu YM, Liu XM and Pan RL. [Research progress on toxic effects of Radix bupleuri] (Chinese). Zhong Chengyao 2012;34:1148-1151
- Lee CH, Wang JD and Chen PC. Risk of liver injury associated with Chinese herbal products containing Radix bupleuri in 639,779 Patients with Hepatitis B virus infection. PLoS One 2011;6:e16064
- Melchardt T, Magnes T, Weiss L, et al. Liver toxicity during temozolomide chemotherapy caused by Chinese herbs. BMC Complement Altern Med 2014;14:115
- Bensky D, Clavey S and Stöger E. Chinese Herbal Medicine. Materia Medica. 3rded. Seattle, WA: Eastland Press, 2004
Aristolochia, „Malignant Lie” or the Bitter Truth?
With medicinal drugs containing Aristolochia banned in many countries all around the world, including China and Taiwan, the Aristolochia-issue should be settled by now. Alas, still a few wrong notions, or a lack of information, towards this problem keep on circulating in the world of TCM.
A comment to the article by Chris Dhaenens 2013, from the Center for Safety of Chinese Herbal Medicine (CTCA) (translated by Angelica Dawson)
Preliminary note: It seems that the story of Aristolochia cannot end on a light note. Actually, it should be part of the past, with medicinal drugs containing Aristolochia banned in many countries all around the world, including China and Taiwan. Alas, still a few wrong notions, or a lack of information, towards this problem keep on circulating in the world of TCM. In 2013 the Belgian Chris Dhaenens published an article relating to this issue in the Journal of the Register of Chinese Herbal Medicine[1]. The background was that critics of phytotherapy kept on holding this story against us. An article in the Lancet Oncology referring to the occurrence of liver injury by arsenic oxide(!), cross-referenced it to the Aristolochia-story without any substantial connection. Notwithstanding his entitlement to criticize this kind of linkage, Chris Dhaenens must be criticized for his display of ignorance towards the problem and downplaying it. Due to his recent republication in German, in the journal Naturheilpraxis (Journal of Natural Healing Practice), the CTCA feels compelled to make a comment. As in this case, we have a definite answer, and the world of TCM must take a clear stand, or face the possibility of being accused of a lack of reality awareness concerning safety issues. As Naturheilpraxis only wanted to provide limited space for our comment in the journal, we had to submit a very condensed version of our article. Below you find the complete wording.
Can the kidney pathology associated with Aristolochia in fact “hardly implicate Aristolochia” and, have the “carcinogenic properties of Aristolochia only been established in rodents”? On the other hand, Chris Dhaenens states “nobody in his right mind disputes the ban of Aristolochia”. How does that fit? These statements in the article display a surprising ignorance and an irresponsible downplaying of the problem. The following will elaborate on the author’s arguments, trying to illustrate, that hardly any phenomenon in medicine has been as clearly demonstrated as the renal toxicity and carcinogenicity of aristolochic acid, contained in relatively potent concentrations in various plants of the Aristolochia genus.
The Belgian slimming clinic
In the Nineties, a Belgium slimming clinic administered a hazardous cocktail of anorectics and other biomedical drugs, mixed with Chinese herbal medicines. When, instead of prescribed Stephaniae tetrandrae Radix (han fang ji), another herb of the Chinese Materia Medica, Aristolochiae fangchi Radix (guang fang ji) was delivered, more than 100 cases of renal injury occurred, the progredient course mostly remaining even after the medication had been discontinued; and roughly 70 percent, with due necessity of dialysis or kidney transplantation[3]. Aristolochia nephropathy (AN) shows itself to be a separate pathological entity with the typical histological picture of interstitial fibrosis and tubular atrophy.
A problem of serotonin?
Chris Dhaenens quotes, that thousands of women have been treated with Aristolochia without occurrence of renal injury; hereby overlooking the vastly different individual reactions to toxins. This kind of phenomenon is also well known with metamizole - only very few of the users develop the dreaded agranulocytosis. Furthermore, the dosage, naturally, plays an important role, in the case of Aristolochia the cumulative dosage, respectively (see below).
Chris Dhaenens assigns the role of the main trigger to serotonin, one of the slimming clinic’s medical cocktail’s components, quoting an editorial from de Broe[4]. But de Broe only writes, that the vaso-constrictive properties of serotonin might have “accelerated or potentiated” the nephrotoxic effects of aristolochic acid which he did not question. He suspects a genetic predisposition to be the cause for only some of the exposed persons developing nephropathy or urothelial cancer. Already several years ago, a dose consideration had suggested the chemical cocktail seemed to function as accelerator in the Belgian cases[5].
Nevertheless, it is futile to criticize the Belgian clinic’s procedure, for without any shadow of doubt, their therapy is medically unacceptable, as well as irresponsible. Anyway, due to the cumulative occurrence of renal injuries, they can “claim credit” for raising the consciousness concerning the nephrotoxicity of Aristolochia.
The effort of dragging forth the Belgian cases with their possible serotonin phenomenon is not necessary at all. Sufficiently enough existing cases of AN have occurred without any influence of serotonin. Multiple hints towards the nephrotoxicity of aristolochic acid, predominantly in animal experiments, had already been given since the fifties[5]. Following the Belgian incidents, many cases of renal injury with the typical feature of AN were uncovered worldwide, occurring first and foremost under usage of Chinese formulae containing Aristolochiae manshuriensis Caulis (guan mu tong) or Aristolochiae fangchi Radix (guang fan ji). The corresponding publications mainly came from Great Britain, France, Taiwan, Japan, China, Hongkong, Korea, Australia, USA and Germany[6]. Another case occurred in Spain, caused by a Western species, Aristolochia pistolochia[7]. These cases led to Aristolochia being banned in many countries including China and Taiwan.
Chinese nephrologists started to routinely check their patients’ case histories of applied drugs in cases of chronic renal disease, especially of the type tubulo-interstitial nephropathy with unclear etiology, after they had received knowledge about the nephrotoxicity of Aristolochia. Within several years, thousands of patients with AN appeared[8]. These facts have been totally edited out by Chris Dhaenens.
Course of Aristolochia nephropathy
Denying and irresponsibly playing down reality, Chris Dhaenens writes, the toxicity of the Aristolochia herb is “acute and reversible”. Such a course is rather the exception - usually the opposite applies. In a Beijing clinic’s department with 58 cases of AN, 4 patients showed an acute form, 7 a so-called tubular dysfunction and 47 a chronic-progressive development[9]. In most patients diagnosed with AN, the disease follows a relatively rapid progress despite discontinuing the Aristolochia medication – according to a Belgian compilation, 83 percent led up to end-stage renal disease within two years[6].
In another department of a Beijing hospital, 300 cases had accumulated over a period of 10 years. Within 3 months after discontinuing the Aristolochia medication, 13 patients showed an acute process, 10 a tubular dysfunction and 280 a chronic development. Amongst the acute cases, only one was reversible; 5 took a progressive course leading to end-stage renal disease. Within the chronic cases, 20 percent showed a partial regression; the renal failure of the other cases progressed, 44 percent quite rapidly with a decline of the glomerular filtration-rate by more than 4 ml/min per year. Most of the patients had taken Aristolochiae manshuriensis Caulis (guan mu tong), followed by Aristolochiae Radix (ging mu xiang), Aristolochiae fangchi Radix (guang fang ji), Aristolochiae debilis Caulis (tian xian teng) and Aristolochiae molissimae Herba (xun gu feng). The contents of aristolochic acid were determined by HPLC, the cumulative dosage correlating with the rapidity of progression within the chronic cases[8].
The carcinogenicity of Aristolochia
The statement that “carcinogenic properties of aristolochic acid could only be found in rodents” is another unbelievable misapprehension of facts. Insights from animal experiments had only been the starting point. 1981 drugs containing aristolochic acid were banned by the Deutsches Bundesgesundheitsamt (German Health-Agency), after a distinct carcinogenicity had been proven experimenting with rats[10].
The Belgian cases showed, more than 40 percent of patients with AN developed malignancies, especially urothelial carcinomas of the upper urinary tract, but also renal cell and bladder carcinomas[11-14]. A current study talks of stringent evidence of the involvement of aristolochic acid in a substantial percentage of renal cell carcinoma cases in Taiwan[15].
A substance’s property of forming DNA-adducts is considered strong evidence for its carcinogenicity. A group of Heidelberg scientists could detect DNA adducts of aristolochic acid, or its metabolite aristolactam in tissue samples of various groups of cancer patients having been treated with Aristolochia herbs. Chris Dhaenens reasons, that these findings had been questioned by another scientist[16]. But DNA-adducts were also verified in numerous cases of cancer associated with aristolochic acid, by other independent researchers from the USA, Croatia and Taiwan[15,17,18]. DNA-adducts could be reproduced in animal-experiments after administering aristolochic acid[19]. In fact, it could be demonstrated, that the mutations in the tumor tissue were frequently triggered in a specific part of a certain gene, the tumor-suppressor gene TP53, that is characteristic for aristolochic acid[17,20]. The mutation deactivates this gene and promotes the development of cancer.
Epidemiological studies in Taiwan
Between 1997 and 2003, up to a third of Taiwan’s population ingested potentially Aristolochia containing medicines[21]; likewise, its population has the highest incidence of end-stage renal disease worldwide. A screening of 199,843 patients, after eliminating confounding influential factors, showed a significantly increased risk of chronic renal disease after ingesting more than 30g mu tong or more than 60g guang fang ji [24].
Another Taiwanese study showed an increased risk of developing urothelial carcinoma in patients with end-stage renal disease, after having ingested mu tong corresponding with an estimated amount of more than 100mg aristolochic acid[25]. It is very rare in medicine that such clear evidence of a substance’s carcinogenic impact can be found, without being dependent on concluding the effect on humans from animal experiments.
Conclusion
For sure, it is annoying, that the Aristolochia problem actually dating from a far back time in Europe, is held against us at every incongruous opportunity. Alas, publications making light of the matter, like the one of Chris Dhaenens, possibly contribute to the adversaries’ justification for opposing Chinese Medicine. Nevertheless - the Aristolochia tragedy being, or rather having been, a disaster for Chinese Medicine, in this respect is a clear exception of the rule. Chinese herbal medicine, competently practiced and with medicines administered in conforming high quality, is a safe therapy. In fact, it has been shown, that patients with a chronic renal disease in Taiwan, who had been treated with Chinese medicines without Aristolochia, manifested a lesser mortality than those without this therapy[26].
Centrum für Therapiesicherheit in der Chinesischen Arzneitherapie (CTCA),
(Center for Safety of Chinese Herbal Medicine (CTCA)), Berlin
References:
1. Dhaenens C. Aristolochia: The malignant lie and the benign truth. J Register Chin Herbal Med 2013;10:39-41
2. Dhaenens C. Aristolochia - die bösartige Lüge und die gutartige Wahrheit. Naturheilpraxis 2016;69:65-8
3. Debelle FD, Vanherweghem JL and Nortier JL. Aristolochic acid nephropathy: a worldwide problem. Kidney Int 2008;74:158-69
4. De Broe ME. On a nephrotoxic and carcinogenic slimming regimen. Am J Kidney Dis 1999;33:1171-3
5. Wiebrecht A. Über die Aristolochia-Nephropathie. Dt Zschr Akupunktur 2000;43:187-97
6. Gökmen MR, Cosyns JP, Arlt VM, et al. The epidemiology, diagnosis, and management of aristolochic acid nephropathy: a narrative review. Ann Intern Med 2013;158:469-77
7. Pena JM, Borras M, Ramos J and Montoliu J. Rapidly progressive interstitial renal fibrosis due to a chronic intake of a herb (Aristolochia pistolochia) infusion. Nephrol Dial Transplant 1996;11:1359-60
8. Yang L, Su T, Li XM, et al. Aristolochic acid nephropathy: variation in presentation and prognosis. Nephrol Dial Transplant 2012;27:292-8
9. Chen W, Chen Y and Li A. [The clinical and pathological manifestations of aristolochic acid nephropathy--the report of 58 cases] (Chinese). Zhonghua Yixue Zazhi 2001; 81:1101-5
10. Hagemann U, Grase R, Thiele A, et al. Probleme der Arzneimittelsicherheit: Aristolochiasäure, Münchner Med Wschr 1982;124:611-2
11. Cosyns JP, Jadoul M, Squifflet J-P, et al. Urothelial lesions in Chinese-herb nephropathy. Am J Kidney Dis 1999;33:1011-7
12. Nortier JL, Martinez M-CM, Schmeiser HH, et al. Urothelial carcinoma associated with the use of a Chinese herb (Aristolochia fangchi). New Engl J Med 2000;342:1686-92
13. Zlotta AR, Roumeguere T, Kuk C, et al. Select screening in a specific high-risk population of patients suggests a stage migration toward detection of non-muscle-invasive bladder cancer. Eur Urol 2011;59:1026-31
14. Lemy A, Wissing KM, Rorive S, et al. Late onset of bladder urothelial carcinoma after kidney transplantation for end-stage aristolochic acid nephropathy: a case series with 15-year follow-up. Am J Kidney Dis 2008;51:471-7
15. Hoang ML, Chen CH, Chen PC, et al. Aristolochic acid in the etiology of renal cell carcinoma. Cancer Epidemiol Biomarkers Prev 2016;25:1600-8
16. Pfohl-Leszkowicz A. Ochratoxin A and aristolochic acid involvement in nephropathies and associated urothelial tract tumours. Arh Hig Rada Toksikol 2009;60:465-83
17. Chen CH, Dickman KG, Moriya M, et al. Aristolochic acid-associated urothelial cancer in Taiwan. Proc Natl Acad Sci U S A 2012;109:8241-6
18. Jelakovic B, Karanovic S, Vukovic-Lela I, et al. Aristolactam-DNA adducts are a biomarker of environmental exposure to aristolochic acid. Kidney Int 2012;81:559-67
19. Dong H, Suzuki N, Torres MC, et al. Quantitative determination of aristolochic acid-derived DNA adducts in rats using 32P-postlabeling/polyacrylamide gel electrophoresis analysis. Drug Metab Dispos 2006;34:1122-7
20. Chen CH, Dickman KG, Huang CY, et al. Aristolochic acid-induced upper tract urothelial carcinoma in Taiwan: clinical characteristics and outcomes. Int J Cancer 2013;133:14-20
21. Hsieh SC, Lin IH, Tseng WL, et al. Prescription profile of potentially aristolochic acid containing Chinese herbal products: an analysis of National Heath Insurance data in Taiwan between 1997 and 2003. BioMed Central 2008;3:1-6
22. Guh JY, Chen HC, Tsai JF and Chuang LY. Herbal therapy is associated with the risk of CKD in adults not using analgesics in Taiwan. Am J Kidney Dis 2007;49:626-33
23. Lai MN, Lai JN, Chen PC, et al. Increased risks of chronic kidney disease associated with prescribed Chinese herbal products suspected to contain aristolochic acid. Nephrology 2009;14:227-34
24. Lai MN, Wang SM, Chen PC, et al. Population-based case-control study of Chinese herbal products containing aristolochic acid and urinary tract cancer risk. J Natl Cancer Inst 2010;102:179-86
25. Wang SM, Lai MN, Wei A, et al. Increased risk of urinary tract cancer in ESRD patients associated with usage of Chinese herbal products suspected of containing aristolochic acid. PLoS One 2014;9:e105218
26. Hsieh CF, Huang SL, Chen CL, et al. Non-aristolochic acid prescribed Chinese herbal medicines and the risk of mortality in patients with chronic kidney disease: results from a population-based follow-up study. BMJ Open 2014;4:e004033
Lu Li and a team of scientists from Hong Kong and Germany published a study (1) comparing the alleged embryotoxicity of ten Chinese herbal medicines according to animal tests with the results of new in vitro tests they carried out. The following herbal medicines were tested for the designated characteristics:
- Tripterygii wilfordii Radix (lei gong teng), considered obsolete due to considerable toxicity;
- Hirudo (shui zhi), the leech, traditionally contraindicated during pregnancy;
- Trichosanthis Radix (tian hua fen), traditionally contraindicated during pregnancy;
- Coptidis Rhizoma (huang lian), contraindicated during pregnancy according to modern research (2);
- Astragali Radix (huang qi), with no known risk during pregnancy;
- Paeoniae Radix (bai shao), with no known risk during pregnancy;
- Scutellariae Radix (huang qin), with no known risk during pregnancy;
- Notoginseng Radix (san qi), traditionally used with caution during pregnancy;
- Carthami Flos (hong hua), contraindicated during pregnancy according to modern research (2).
- Salviae miltiorrhizae Radix (dan shen) is traditionally contraindicated during pregnancy due to the risk of miscarriage.
First, these herbal medicines were categorized according to their presumed level of embryotoxicity, as described in the literature: strong, weak, or non-existent. However, these classifications are incorrect in several respects. Tripterygii wilfordii Radix (lei gong teng) and Hirudo (shui zhi) are accurately classified as strongly embryotoxic. However, for Trichosanthis Radix (tian hua fen), which is also classified as strongly embryotoxic, no usable data applicable to a decoction or granules exists. The study by Li et al. presents data on trichosanthin, a protein isolated from Trichosanthis Radix that has a strong abortifacient effect and has been used clinically by injection for this purpose. This application has been discontinued due to frequent allergic reactions. In addition to being abortifacient, trichosanthin displayed embryotoxic and teratogenic effects in animal tests. The protein is probably denatured by heat, which might render it ineffective. Although embryotoxic risk cannot be ruled out, these data cannot be applied to a whole extract of Trichosanthis Radix derived from a decoction. The available data cannot confirm or exclude the embryotoxicity of Trichosanthis Radix.
Similarly, the data on Astragali Radix (huang qi) is inconclusive regarding possible embryotoxicity. So far, animal-testing-based studies only exist relating to the substance astragaloside IV. In rabbits and/or rats, there was an increased number of stillbirths, as well as developmental retardation in some cases, though no malformations were observed (3-6). Based on these data, it is not possible to formulate a statement regarding the whole extract of Astragali Radix.
Coptidis Rhizome (huang lian) is described by Li et al., based on literature data, as "weakly embryotoxic." Chuang et al.'s comparatively minor study (7) shows a slight, non-significant decrease in birth weight of newborns. Yet, a crucial study by the same authors (8) demonstrating a significant risk of malformation when mothers took this medicine during the first trimester of pregnancy is ignored. Therefore, Coptidis Rhizome has to be considered strongly embryotoxic, particularly due to the existence of human data.
Paeoniae Radix Alba (bai shao) is considered to have a low risk of embryotoxicity; however, no literature references are provided. A decoction of the medicine showed no embryotoxic or teratogenic effects in mice, a test on stem cells revealed no significant cytotoxicity (9).
A lack of embryotoxicity for Scutellariae Radix (huang qin), Notoginseng Radix (san qi) and Salviae miltiorrhizae Radix (dan shen) is compatible with the literature. On the other hand, the pronounced embryotoxicity of Carthami Flos (hong hua) was not acknowledged. A decoction or aqueous extract of this medicine showed, as well as a higher rate of miscarriage, an increased rate of stillbirths, delays in fetal development and deformities in rats (10, 11). In mice, there was an increased incidence of embryo death and likewise a higher rate of stillbirths and deformities (12, 13).
Thus much of the information on allegedly known embryotoxicity of the 10 herbal medicines represents either an under- or overestimate; in two cases an evaluation is not possible due to a lack of meaningful data. The study by Li et al. used various in vitro tests for determining the embryotoxicity of these medicines, and compared their results with the (allegedly) known embryotoxicity from in vivo tests. In vitro methods offer the advantage of sparing experimental animals. The question is, how well can they predict embryotoxicity risk and/or to what extent do their results correlate with those of in vivo tests. Table: Comparison of in vivo embryotoxicity according to the literature (alleged and actual) with the in vitro results of various test procedures by Li et al. (1).
The study group applied three different testing systems: the embryonic stem cell test (EST), the micromass (MM) and the whole embryo culture (WEC) in two forms: WEC (PM1) and WEC (PM2). An overview of the alleged and the actual known in vivo embryotoxicity, as well as the embryotoxicity prediction from the various in vitro tests is shown in the table. For the medicines Trichosanthis Radix (tian hua fen) and Astragali Radix (huang qi), no information regarding known embryotoxicity can be given, as no valid data exist. It is evident that many of the in vitro results differ from previously known risk data. The strong embryotoxicity of Hirudo is only identified as such in 2 out of 4 tests, that of Coptidis Rhizoma in only 1 out of 4; the well-documented strong embryotoxicity of Carthami Flos is not detected as such at all. On the other hand, the results of several in vitro tests indicate weak embryotoxicity for medicines to which none had previously been attributed.
Conclusion
The study by Li et al. does not accurately reflect previously known in vivo embryotoxicity. The pronounced embryotoxicity of Coptidis Rhizoma and Carthami Flos is underestimated or negated. The alleged weak embryotoxicity of Paeoniae Radix Alba is not substantiated and contradicts data from the literature. Numerous errors in citations, quoted numerical data, and units that differ from the literature will not be addressed in detail here. The in vitro test procedures presented are an interesting contribution. However, their results for eight herbal medicines bear limited correlation to previously known results from the literature. The extent to which in vitro tests for the reproductive toxicity of Chinese herbal medicines can replace in vivo studies requires further research.
Axel Wiebrecht
References
- Li L, Yin Tang L, Liang B, et al. Evaluation of in vitro embryotoxicity tests for Chinese herbal medicines. Reprod Toxicol. 2019;89:45-53.
- Wiebrecht A. Sicherheit in der Chinesischen Arzneitherapie. In: Focks C, ed. Leitfaden Chinesische Medizin. 7thed. München: Elsevier; 2017:978-1028,1160-1164.
- Zhu JB, Zhu YP, Zhang TG. [Evaluation of toxicity of astragaloside IV in rats and rabbits] (Chinese). Du Lixue Zazhi [Journal of Toxicology]. 2007;21(4):317-318.
- Zhu JB, Wan XY, Zhu YP, et al. Effect of astragaloside IV on the embryo-fetal development of Sprague-Dawley rats and New Zealand White rabbits. J Appl Toxicol. 2009;29(5):381-385.
- Zhu YP, Zhang TB, Wan XY, et al. [Study on the teratogenicity of astragaloside IV in SD rats] (Chinese). Zhong Chengyao [Chinese Traditional Patent Medicine]. 2010;32(10):1783-1785.
- Wan XY, Zhu JB, Zhu YP, et al. Effect of astragaloside IV on the general and peripartum reproductive toxicity in Sprague-Dawley rats. Int J Toxicol. 2010;29(5):505-516.
- Chuang CH, Lai JN, Wang JD, et al. Use of Coptidis Rhizoma and foetal growth: a follow-up study of 9,895 pregnancies. Pharmacoepidemiol Drug Saf. 2006;15(3):185-192.
- Chuang CH, Doyle P, Wang JD, et al. Herbal medicines used during the first trimester and major congenital malformations: an analysis of data from a pregnancy cohort study. Drug Saf. 2006;29(6):537-48.
- Xu W, Xu L, Deng B, et al. The potential impact of Radix Paeoniae alba in embryonic development of mice. Phytother Res. 2017;31(9):1376-1383.
- Lin BH, Yan DP, Zhou LR, et al. [Toxicity and effects of Flos Carthami on rat pregnancy and embryonic development] (Chinese). Anhui Zhongyi Xueyuan Xuebao [Journal of Anhui University of Chinese Medicine]. 1998;17(4):50-52.
- Zhao YL, Feng B, Zhou Y, Zhang J. [Study on selective expression of toxicity of Flos Carthami in pregnant rats] (Chinese). Liaoning Zhongyi Zazhi [Liaoning Journal of TCM]. 2011;38(11):2274-2276.
- Nobakht M, Fattahi M, Hoormand M, et al. A study on the teratogenic and cytotoxic effects of safflower extract. J Ethnopharmacol. 2000;73(3):453-459.
- Song XQ, Li JH, Wei HP, et al. [Effects of Flos Carthami on estrogen/progesterone and their receptors in early pregnancy of mice] (Chinese). Zhongguo Xiandai Yixue Zazhi [China Journal of Modern Medicine]. 2014;24(32):5-8.
A new study on liver injury caused by Chinese herbal medicines: substantial data, questionable conclusions
Dec, 2017, slightly modified Jun, 2026
The study
A recent study by Melchart and co-authors [1] analysed the incidence of liver injuries occurring in an TCM hospital in Kötzting, Germany from 1994 to 2015. Included were patients treated with Chinese herbal therapy whose liver enzyme ALT (alanine aminotransferase) at the time of admission was within the normal range. Just before discharge, the liver function was checked again. An elevation of ALT up to 5 times the upper norm was considered as an adaptive phenomenon of the liver, and a higher increase was interpreted as liver injury. The average treatment time was 19.5 days due to the duration of inpatient stay. The association of liver injury with the Chinese medicines was assessed using the internationally accepted RUCAM (or CIOMS) scale [7].
21,740 patient cases were evaluated. An ALT elevation above the normal range was observed in 3.93% of cases, and liver injury with an at least 5-fold ALT elevation occurred in 26 patients (0.12%). In 8 out of these 26 patients, the authors stated a "probable" association with Chinese herbs, in 16 cases a "possible" association, and in 2 cases they excluded a causality. Bupleuri Radix (chai hu) and Scutellariae Radix (huang qin) particularly stand out, as they were involved in 7 of the "probable" or "possible" cases, in 6 of which both were involved simultaneously.
In their analysis, the authors supposed a known hepatotoxicity for a number of herbs („associated with potential liver injury as evidenced from the scientific literature“) which were involved in the cases, namely Bombyx batryticatus (jiang can), Dictamni cortex (bai xian pi), Ephedrae herba (ma huang), Glycyrrhizae radix (gan cao), Polygoni multiflori caulis (shou wu teng), Polygoni multiflori radix (he shou wu), Polygoni cuspidati rhizoma (hu zhang), Psoraleae fructus (bu gu zhi), Puerariae radix (ge gen), Rhei radix et rhizoma (da huang), Sennae folium* (fan xie ye) and Toosendan fructus* (chuan lian zi).
*Name has been adjusted to the current nomenclature.
Commentary
This study provides valuable, unprecedented data for assessing the potential risk of Chinese herb-induced liver injury, characterised by the following features:
- the prospective design
- the high number of 21,470 included patients which allows a valid estimate of the incidence of liver injuries in non-predisposed patients within a limited period of time (19.5 days on average)
- the prior authentication and testing for contamination of the herbs used
- reference to European conditions by exclusion of prohibited substances, the most toxic medicinals which are uncommon in this area, and the use of excessively high doses
- and last but not least, full transparency regarding all components of the herbal formulas and the calculation of the RUCAM scores.
This is thanks to the authors. An important signal is that relevant liver injury caused by Chinese herbs - at least under the conditions of the study - rarely occurs, and after the discontinuation of therapy, usually regresses uneventfully. However, with regard to the interpretation of the results, some comments and corrections to the study appear to be appropriate.
In evaluating the causality between certain herbs and an observed liver injury, the extent to which hepatotoxicity is already considered proven for these herbs is a key point. Known hepatotoxicity leads to an increase of 1 to 2 points in the probability of a causality concerning the RUCAM score used in the study. These points often make the difference between a "possible" and a "probable" association or if one herb or another is suspected of being the causative agent. If an assumption is made without sufficient evidence, one runs the risk of confirming prejudices and reproducing misconceptions. Frequent repetitions do not make statements more true. In addition, evidence of causality assignment can only rely on "probable" or "very probable" associations to avoid misjudgements. "Possible" associations may have a supportive role or may draw attention to certain herbs, but they can not establish evidence.
For several herbs, which were suspected of being hepatotoxic in the study, these reservations are relevant. The most striking example is Glycyrrhizae radix. This is the herb most commonly used in Chinese medicine which is contained in approximately 50% of herbal formulas. If a formula is suspected of liver toxicity, then Glycyrrhizae radix is automatically involved in about half of the cases. The same also applies to other herbs commonly used in Chinese medicine such as Atractylodis macrocephalae rhizoma or Angelica sinensis radix. Therefore, the suspicion is justified only if the involvement of a herb in liver injury is significantly higher than its average frequency of use. Reservation should be used when a particular herb is involved that commonly is prescribed together with a potentially hepatotoxic agent, because both substances are indicated for certain diseases or their effects complement each other. Here, the frequent involvement of a herb can create a wrong picture.
In a previous smaller study from the Kötzting hospital [2], Glycyrrhizae radix and Atractylodis macrocephalae rhizoma stood out significantly as ingredients of herbal formulas associated with liver enzyme elevations. The authors had described these results as possibly due to chance or to confounding factors, since these herbs had not previously been reported as hepatotoxic in the literature. In the current study, Glycyrrhizae radix and Atractylodis macrocephalae rhizoma are involved in only 2 out of 9 cases as being "probably" associated with liver injury, whereupon the inclusion criterion is not based on a 2-fold, but on a more than 5-fold elevation of ALT above upper norm. Nevertheless, a suspected hepatotoxicity for Glycyrrhizae radix in the present study is stated because this property is assumed as being established.
One contributing author repeatedly stressed a hepatotoxicity of Glycyrrhizae radix (gan cao) as having been documented in the literature [3-5] which increased the likelihood of it being associated with liver injury in the present study according to the RUCAM test by 2 points. This assessment is based on two poorly documented case reports within a single publication from Hong Kong [6]. One of these two case reports is sufficient for Teschke and co-authors [3, 5] to establish the hepatotoxicity of three herbs simultaneously, which is hard to reconcile with the laws of logic. The rationale was that the hepatotoxicity of the herbs should be apparently known, but references are not provided by either the authors of the case reports or by Teschke et al. A complete account of the ingredients used in the herbal formulas was missing, as well as the authentication of the herbs or testing for contaminants. The accepted and widely used procedure for assessing the causality of drug-related liver injury is the RUCAM (or CIOMS) test [7]. The scores cited by Teschke et al. [3] for the RUCAM tests are fictitious; the tests were not performed properly. A recalculation resulted in a RUCAM score of 2 or 3 instead of "6 to 8" for the herbs in question, so that the causality is "unlikely" or even "possible" [8]. Thus, these case reports are not appropriate for establishing hepatotoxicity. There is no evidence of hepatotoxicity relating to Glycyrrhizae radix.
Another case is Bombyx batryticatus. Here too, without legitimacy, the authors claim hepatotoxicity as being known. In many larger case compilations of liver injury, this medicine is missing [9-19]. In the publication by B. Shaw [20], Bombyx batryticatus was present, as an ingredient of the complex formulas, in just 2 out of 40 patients with a liver reaction likely or possibly related to Chinese herbal medicine, without it being cause for suggesting a suspected hepatotoxicity. The review by Tu et al. [21] gives a detailed report on the side effects of Bombyx batryticatus, with no mention of liver toxicity. If you search for "Bombyx" and "(liver injury or hepatotoxicity)" in Pub Med, you will find 3 publications that describe a hepatoprotective property of this herb. The work by Teschke et al. [22], which in turn relies merely on the unsuitable Hong Kong case study [6], stands alone in asserting a potential hepatotoxicity.
For a valid causality assessment, clear evidence for the assumption of a "known" hepatotoxicity is required. Herbal medicines, especially those from TCM, involve a particular challenge: they are rarely used as single herbs. In multicomponent herbal formulas, it is difficult to blame a particular ingredient for the reaction. The identity of the herbs must be ensured, since mistakes or deliberate adulterations do occur. Furthermore, contamination due to impurities, undesirable substances or conventional drugs must be excluded. The way in which a herb is prepared or pre-treated, which is often done just to reduce toxicity, can also play a crucial role [9]. Therefore, one cannot unconditionally apply study results from another therapeutic system (e.g., Kampo, Ayurveda) which uses a different method of preparation, to TCM.
The conditions for evidence are fulfilled by only a few herbs. For Polygoni multiflori radix (he shou wu), they are beyond doubt. It is often used as a single herb, too. Among the numerous case reports, authentication or testing for contaminants was partially carried out. For Dictamni cortex (bai xian pi), there are only a few cases of it being used as a single herb [23, 24]. However, it is striking that this herb is significantly more probable to be involved in liver injury than its frequency of use accounts for.
Other herbs with insufficiently documented evidence, which are considered potentially hepatotoxic in the study, are: Sennae folium, Polygoni cuspidati rhizoma, Polygoni multiflori caulis, Pueraria radix and Rhei radix et rhizoma. For example, with Puerariae radix: Teschke et al. [22] cited a reference dealing with two cases of hepatitis due to the juice of Puerariae lobatae radix from Korea [25]. An authentication of the preparations was not documented. The phytochemical composition of the juice cannot be equated with that of a decoction from the dried root as it is used in the context of Chinese medicine. The RUCAM tests which were carried out, each with a high score of 10 [25], are not credible since the differential diagnosis is incomplete and the documentation of the quo ante hepatotoxicity is not sufficiently substantiated.
The updated RUCAM test assigns two points for hepatotoxicity if it is listed in the product characteristic, and one point if there is only evidence in the literature [7]. A product characteristic is missing for raw herbs. TCM finished products with a single herb as the active ingredient exist only as an exception. For the assured, albeit very rare, hepatotoxicity of Polygoni multiflori radix (he shou wu), 2 points can be applied analogously. For other herbs that are mentioned in publications, but for which there is no clear evidence, a rating with a quo-ante score of "1" is appropriate: this applies for Ephedrae herba, Toosendan fructus, Bupleuri radix and Scutellariae radix. For the remaining herbs mentioned in the study, no valid references have been documented which would justify one point.
In several cases, this approach leads to an amendment of the RUCAM assessment (Table 1). Of the 9 study cases whose association with Chinese medicine should be "probable", only 4 remain: cases 3, 12, 14 and 19.2; each with a RUCAM score of 6. This "probable" association applies to the entire herbal formula and can only be applied to a single herb if not more than one ingredient of the formula is suspected of being hepatotoxic. This is true for case no. 12, where only Toosendan fructus with a score of "1" justifies a RUCAM score of 6 for a "probable" association. The RUCAM test states that if other substances are eligible as an alternative cause, "2" points should be deducted [7]. If 2 or more herbs with a pre-existing suspicion of hepatotoxicity are involved, then, if you want to break down the causality to the individual herbs, these 2 points should be subtracted. Then, a "probable" causality can no longer be assumed for these single herbs.
| Fall Nr. | 3 | 4 | 12 | 14 | 17 | 18 | 19(1) | 19(2) | 24 |
|---|---|---|---|---|---|---|---|---|---|
| RUCAM lt. Melchart et al. | 7 | 6 | 7 | 7 | 6? | 6 | 6 | 7 | 6? |
| Zeit bis zur Reaktion | 2 | 2 | 2 | 2 | 2 | 2? | 1→2 | 1→2 | 2 |
| Rückgang der ALT | 2 | 2 | 2 | 3 | 3→2 | 2→0 | 1→3 | 1→3 | 2 |
| Alkoholkonsum | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Alter >55 | 1 | 1 | 1 | 1 | |||||
| Begleitdrogen/-arzneimittel | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| alternative Ursachen | 0→-2 | 0→-2 | 0→-2 | 0 | 0 | 0 | 1→-2 | 1→-2 | -2 |
| vorliegende Inform. ü. Hepatotoxizität | 2→1 | 2→1 | 2→1 | 2→1 | 2→1 | 2→1 | 2→1 | 2→1 | 2→1 |
| Reexposition | 1 | ||||||||
| RUCAM revidiert | 4 | 3 | 4 | 6 | 5 | 3 | 5 | 6 | 3 |
| beteiligte Drogen | |||||||||
| Bupleuri rd. (chai hu) | x | x | x | x | x | x | x | ||
| Scutellariae rd. (huang qin) | x | x | x | x | x | x | x | ||
| Ephedrae hb. (ma huang) | x | x | |||||||
| Toosendan fr. (chuan lian zi) | x | x |
Tab. 1: RUCAM scores and their composition acc. to Melchart et al. (black) and revisions based on the reevaluation (red). In Case 19(2), the patient was re-exposed to certain medicines after 3 years. The scores refer to the decoction as a whole; to assess the individual medicines, the probability score must be reduced by 1 point in each case. Interpretation of the RUCAM score: >8 points: “very likely”, 6–8 points: “likely”, 3–5 points: “possible”, <3 points: unlikely, excluded, or cannot be assessed.
Bupleuri radix and Scutellariae baicalensis Radix deserve special consideration. There is an abundance of cases of hepatotoxicity in Kampo medicine for formulas containing these substances. Mostly often, both herbs are used simultaneously, e.g. in the formula sho-saiko-to (corresponding to xiao chai hu tang). In Chinese medicine, however, liver injury due to these herbs is scarcely known [26]. Kampo herbs are not simply comparable to those of Chinese medicine. For Bupleuri radix, the species Bupleurum falcatum is used in Kampo medicine [27]. In Chinese medicine, the species B. chinense or B. scorzonerifolium are officinal [28]. In Japan, standard formulas are predominantly used as granules. Alcohol can also be part of the extraction solvent [27], which means that the composition of the extracts is not comparable to that of decoctions from Chinese medicine. As to acute toxicity testing, an ethanol extract was more toxic to the liver than an aqueous extract [29].
Within Chinese medicine, there have been only sporadic case reports with inadequate causality criteria [30, 31] in which these herbs appeared. For the first time, the present study documents several cases with formulas containing Bupleuri radix and Scutellariae radix associated with liver injury, where testing for identity and contamination was done. In the 4 cases remaining as "probable" after revision, Bupleuri radix is involved twice and Scutellariae radix three times. In case 3, where both herbs are involved, Ephedrae herba appears as an alternative causative agent, and in case 14 (without Bupleuri radix), the potential causative agent Toosendan fructus is present. A clear assignment to Bupleuri radix or Scutellariae radix is therefore not possible so far. In case 19.2, only these two herbs are present with a potential quo-ante suspicion. Of particular importance here is the patient's rechallenge by a formula which again contained both of these herbs, but only 3 other herbs (Curcumae longae rhizoma, Curcumae radix and Mori ramulus), which were given in the first formula and for which no reasonable suspicion exists. In addition, it is peculiarly striking how many cases with a “possible” causality these two herbs were involved in.
Based on this new data quality, one has to reassess the hepatotoxicity of Bupleuri radix and Scutellariae radix. Either one herb or the other, or both herbs together, should be considered to be potentially hepatotoxic. However, a definite allocation of causality to one or the other herb does not appear to be feasible without reservation according to the current level of evidence. When using either one of these herbs, one must be prepared for the very rare possibility of an idiosyncratic (unpredictable) reaction.
A re-evaluation also seems appropriate for Toosendan fructus. So far, a possible hepatotoxicity only applied in the case of overdose [32]. Now, the herb is implicated in two out of four cases with a probable association; in case 12, without any other suspected herbs included in the formula. Apparently, hepatotoxicity can also occur in the normal dose range. Unfortunately, dosages are not detailed in this study. However, if there is a dose-dependency, it may be more of an intrinsic hepatotoxicity that could be controlled by limiting the dosage.
For a reassessment of Ephedrae herba, the results of the study are not sufficient. This herb is involved in case 3 in which Bupleuri radix and Scutellariae radix are present, so a clear assignment is not possible. The same applies to case 7 and the first formula in case 19 (19.1), for which the association is merely "possible"; in case 20, Bupleuri radix was used simultaneously. The limited number of hepatotoxicity cases involving Ephedra herba documented in the literature must be weighed against the millions of times the drug was used as a dietary supplement, especially in the years previous to 2004. However, with the cases from the present study, this herb shifts into the upper range of a "possible" hepatotoxicity.
Conclusion
The study contains unprecedented data quality for assessing the hepatotoxic risk of Chinese herbal medicines. However, many of the evaluations made in the publication do not hold up. The potential hepatotoxicity of Bupleuri radix or Scutellariae baicalensis radix, or of a combination of both drugs together in the context of Chinese medicine must be deemed adequately secured although a further differentiation currently is not possible. Toosendan fructus, at standard dosages, also appears to be possibly hepatotoxic even though the dosages were not explicitly reported in the respective cases of the study. The possible liver injury caused by Polygoni multiflori radix has already been confirmed, and the study provides no additional support on this. Toxicity cases involving this herb seem to be less common in Western countries than in Asia.
Overall, liver injuries caused by Chinese herbal medicine are very rare and their prognosis, if recognized early enough, is generally uneventful. For a duration of use longer than 19.5 days, as in the present study, the incidence might be higher than reported here. If liver reactions associated with Chinese herbal medicine occur, it is advisable to carry out a full differential diagnostic procedurefull differential diagnostic procedure to either confirm or disprove the causality, so that the evidence regarding Chinese herbs and their actual hepatotoxic risks increases. This applies not only to the Kötzting hospital, but in every case. The Centre for Safety of Chinese Herbal Medicines, CTCA (Centrum für Therapiesicherheit in der Chinesischen Arzneitherapie) is an appropriate address for dealing with this matter.
Literature:
- Melchart D, Hager S, Albrecht S, Dai J, Weidenhammer W and Teschke R. Herbal Traditional Chinese Medicine and suspected liver injury: A prospective study. World J Hepatol 2017;9:1141-1157
- Melchart D, Linde K, Hager S, et al. Monitoring of liver enzymes in patients treated with traditional Chinese drugs. Complement Ther Med 1999;7:208-216
- Teschke R, Zhang L, Long H, et al. Traditional Chinese Medicine and herbal hepatotoxicity: a tabular compilation of reported cases. Ann Hepatol 2015;14:7-19
- Teschke R, Wolff A, Frenzel C and Schulze J. Review article: herbal hepatotoxicity - an update on traditional Chinese medicine preparations. Aliment Pharmacol Ther 2014;40:32-50
- Teschke R, Larrey D, Melchart D and Danan G. Traditional Chinese Medicine (TCM) and herbal hepatotoxicity: RUCAM and the role of novel diagnostic biomarkers such as MicroRNAs. Medicines 2016;3:18
- Yuen MF, Tam S, Fung J, et al. Traditional Chinese medicine causing hepatotoxicity in patients with chronic hepatitis B infection: a 1-year prospective study. Aliment Pharmacol Ther 2006;24:1179-1186
- Danan G, Teschke R. RUCAM in drug and herb induced liver injury: The update. Int J Mol Sci 2015;17:E14
- 8. Wiebrecht A. Dubious pseudoscience – on the alleged hepatotoxicity of Chinese herbal medicines.Bitte link setzen zu: https://www.ctca.center/de/stellungnahmen/kommentare.html
- Teo DC, Ng PS, Tan SH, et al. Drug-induced liver injury associated with Complementary and Alternative Medicine: a review of adverse event reports in an Asian community from 2009 to 2014. BMC Complement Altern Med 2016;16:192
- Chen YF, Cai HD. [Investigation of liver damage associated with Chinese medicines] (Chinese). Yaowu Buliang Fanying Zazhi 1999;1:27-32
- Li XY, Li CQ, Zhang ZM, et al. [Study on traditional Chinese medicine-induced liver injury: from theory to clinical analysis] (Chinese). Zhuanhua Yixue Zazhi 2015;4:244-249
- Chau TN, Cheung WI, Ngan T, et al. Causality assessment of herb-induced liver injury using multidisciplinary approach and Roussel Uclaf Causality Assessment Method (RUCAM). Clin Toxicol2011;49:34-39
- Lee WJ, Kim HW, Lee HY and Son CG. Systematic review on herb-induced liver injury in Korea. Food Chem Toxicol 2015;84:47-54
- Ma X, Peng JH and Hu YY. Chinese Herbal Medicine-induced Liver Injury. J Clin Transl Hepatol 2014;2:170-175
- 1Peng XL, Li CS and Cui SZ. [Biometrical analysis on liver injury caused by traditional Chinese herbs] (Chinese). Shizhen Guoyi Guoyao 1999;10:392-393
- Pittler MH, Ernst E. Systematic review: hepatotoxic events associated with herbal medicinal products. Aliment Pharmacol Ther 2003;18:451-471
- Zhang P, Ye Y, Yang X and Jiao Y. Systematic review on Chinese herbal medicine induced liver injury. Evid Based Complement Alternat Med 2016;2016:3560812
- Zhao P, Wang C, Liu W and Wang F. Acute liver failure associated with traditional Chinese medicine: report of 30 cases from seven tertiary hospitals in China. Crit Care Med 2014;42:e296-299
- Wang XJ, Xu LP and Wang M. [Hepatotoxicity caused by commonly used Chinese medicinal herbs and compound preparations] (Chinese). Shoudu Yike Daxue Xuebao 2007;28:220-224
- Shaw BJ. Aspects of Chinese herbal medicine with relation to their hepatotoxicity. A thesis submitted to King's College London for the degree of Doctor of Philosophy. School of Biomedical and Health Sciences, King's College London & Royal Botanical Gardens, Kew, 2007
- Tu YD, Yu XP. [The clinical use of Bambusa textilis in lung diseases and its side effects] (Chinese). Shanghai Zhongyiyao Zazhi 2012;46:64-66
- Teschke R. Traditional Chinese Medicine induced liver injury. J Clin Translat Hepatol 2014;2:80-94
- Lee JH, Lee HY, Koh KC, et al. [Drug induced liver disease caused by ingestion of Dictamnus dasycarpus] (Korean). Korean J Gastroenterol 1998;31:251-257
- Jang JS, Seo EG, Han C, et al. [Four cases of toxic liver injury associated with Dictamnus dasycarpus] (Korean). Korean J Hepatol 2008;14:206-212
- Kim SY, Yim HJ, Ahn JH, et al. [Two cases of toxic hepatitis caused by arrowroot juice] (Korean). Korean J Hepatol 2009;15:504-509
- Wu SX, Sun HF, Yang XH, et al. ["Re-evaluation upon suspected event" is an approach for post-marketing clinical study: lessons from adverse drug events related to Bupleuri Radix preparations] (Chinese). Zhongguo Zhongyao Zazhi 2014;39:2983-2988
- Japanese Pharmacopoeia (JP XVI). English Version. 16th ed. Tokyo: Pharmaceutical and Medical Device Regulatory Science Society of Japan, 2012
- Chinese Pharmacopoeia Commission. Pharmacopoeia of the Peoples Republic of China (English version). Vol. I. Beijing, China: China Medical Science Press, 2015
- Liu YM, Liu XM and Pan RL. [Research progress on toxic effects of Radix bupleuri] (Chinese). Zhong Chengyao 2012;34:1148-1151
- Lee CH, Wang JD and Chen PC. Risk of liver injury associated with Chinese herbal products containing Radix bupleuri in 639,779 Patients with Hepatitis B virus infection. PLoS One 2011;6:e16064
- Melchardt T, Magnes T, Weiss L, et al. Liver toxicity during temozolomide chemotherapy caused by Chinese herbs. BMC Complement Altern Med 2014;14:115
- Bensky D, Clavey S and Stöger E. Chinese Herbal Medicine. Materia Medica. 3rded. Seattle, WA: Eastland Press, 2004
With medicinal drugs containing Aristolochia banned in many countries all around the world, including China and Taiwan, the Aristolochia-issue should be settled by now. Alas, still a few wrong notions, or a lack of information, towards this problem keep on circulating in the world of TCM.
A comment to the article by Chris Dhaenens 2013, from the Center for Safety of Chinese Herbal Medicine (CTCA) (translated by Angelica Dawson)
Preliminary note: It seems that the story of Aristolochia cannot end on a light note. Actually, it should be part of the past, with medicinal drugs containing Aristolochia banned in many countries all around the world, including China and Taiwan. Alas, still a few wrong notions, or a lack of information, towards this problem keep on circulating in the world of TCM. In 2013 the Belgian Chris Dhaenens published an article relating to this issue in the Journal of the Register of Chinese Herbal Medicine[1]. The background was that critics of phytotherapy kept on holding this story against us. An article in the Lancet Oncology referring to the occurrence of liver injury by arsenic oxide(!), cross-referenced it to the Aristolochia-story without any substantial connection. Notwithstanding his entitlement to criticize this kind of linkage, Chris Dhaenens must be criticized for his display of ignorance towards the problem and downplaying it. Due to his recent republication in German, in the journal Naturheilpraxis (Journal of Natural Healing Practice), the CTCA feels compelled to make a comment. As in this case, we have a definite answer, and the world of TCM must take a clear stand, or face the possibility of being accused of a lack of reality awareness concerning safety issues. As Naturheilpraxis only wanted to provide limited space for our comment in the journal, we had to submit a very condensed version of our article. Below you find the complete wording.
Can the kidney pathology associated with Aristolochia in fact “hardly implicate Aristolochia” and, have the “carcinogenic properties of Aristolochia only been established in rodents”? On the other hand, Chris Dhaenens states “nobody in his right mind disputes the ban of Aristolochia”. How does that fit? These statements in the article display a surprising ignorance and an irresponsible downplaying of the problem. The following will elaborate on the author’s arguments, trying to illustrate, that hardly any phenomenon in medicine has been as clearly demonstrated as the renal toxicity and carcinogenicity of aristolochic acid, contained in relatively potent concentrations in various plants of the Aristolochia genus.
The Belgian slimming clinic
In the Nineties, a Belgium slimming clinic administered a hazardous cocktail of anorectics and other biomedical drugs, mixed with Chinese herbal medicines. When, instead of prescribed Stephaniae tetrandrae Radix (han fang ji), another herb of the Chinese Materia Medica, Aristolochiae fangchi Radix (guang fang ji) was delivered, more than 100 cases of renal injury occurred, the progredient course mostly remaining even after the medication had been discontinued; and roughly 70 percent, with due necessity of dialysis or kidney transplantation[3]. Aristolochia nephropathy (AN) shows itself to be a separate pathological entity with the typical histological picture of interstitial fibrosis and tubular atrophy.
A problem of serotonin?
Chris Dhaenens quotes, that thousands of women have been treated with Aristolochia without occurrence of renal injury; hereby overlooking the vastly different individual reactions to toxins. This kind of phenomenon is also well known with metamizole - only very few of the users develop the dreaded agranulocytosis. Furthermore, the dosage, naturally, plays an important role, in the case of Aristolochia the cumulative dosage, respectively (see below).
Chris Dhaenens assigns the role of the main trigger to serotonin, one of the slimming clinic’s medical cocktail’s components, quoting an editorial from de Broe[4]. But de Broe only writes, that the vaso-constrictive properties of serotonin might have “accelerated or potentiated” the nephrotoxic effects of aristolochic acid which he did not question. He suspects a genetic predisposition to be the cause for only some of the exposed persons developing nephropathy or urothelial cancer. Already several years ago, a dose consideration had suggested the chemical cocktail seemed to function as accelerator in the Belgian cases[5].
Nevertheless, it is futile to criticize the Belgian clinic’s procedure, for without any shadow of doubt, their therapy is medically unacceptable, as well as irresponsible. Anyway, due to the cumulative occurrence of renal injuries, they can “claim credit” for raising the consciousness concerning the nephrotoxicity of Aristolochia.
The effort of dragging forth the Belgian cases with their possible serotonin phenomenon is not necessary at all. Sufficiently enough existing cases of AN have occurred without any influence of serotonin. Multiple hints towards the nephrotoxicity of aristolochic acid, predominantly in animal experiments, had already been given since the fifties[5]. Following the Belgian incidents, many cases of renal injury with the typical feature of AN were uncovered worldwide, occurring first and foremost under usage of Chinese formulae containing Aristolochiae manshuriensis Caulis (guan mu tong) or Aristolochiae fangchi Radix (guang fan ji). The corresponding publications mainly came from Great Britain, France, Taiwan, Japan, China, Hongkong, Korea, Australia, USA and Germany[6]. Another case occurred in Spain, caused by a Western species, Aristolochia pistolochia[7]. These cases led to Aristolochia being banned in many countries including China and Taiwan.
Chinese nephrologists started to routinely check their patients’ case histories of applied drugs in cases of chronic renal disease, especially of the type tubulo-interstitial nephropathy with unclear etiology, after they had received knowledge about the nephrotoxicity of Aristolochia. Within several years, thousands of patients with AN appeared[8]. These facts have been totally edited out by Chris Dhaenens.
Course of Aristolochia nephropathy
Denying and irresponsibly playing down reality, Chris Dhaenens writes, the toxicity of the Aristolochia herb is “acute and reversible”. Such a course is rather the exception - usually the opposite applies. In a Beijing clinic’s department with 58 cases of AN, 4 patients showed an acute form, 7 a so-called tubular dysfunction and 47 a chronic-progressive development[9]. In most patients diagnosed with AN, the disease follows a relatively rapid progress despite discontinuing the Aristolochia medication – according to a Belgian compilation, 83 percent led up to end-stage renal disease within two years[6].
In another department of a Beijing hospital, 300 cases had accumulated over a period of 10 years. Within 3 months after discontinuing the Aristolochia medication, 13 patients showed an acute process, 10 a tubular dysfunction and 280 a chronic development. Amongst the acute cases, only one was reversible; 5 took a progressive course leading to end-stage renal disease. Within the chronic cases, 20 percent showed a partial regression; the renal failure of the other cases progressed, 44 percent quite rapidly with a decline of the glomerular filtration-rate by more than 4 ml/min per year. Most of the patients had taken Aristolochiae manshuriensis Caulis (guan mu tong), followed by Aristolochiae Radix (ging mu xiang), Aristolochiae fangchi Radix (guang fang ji), Aristolochiae debilis Caulis (tian xian teng) and Aristolochiae molissimae Herba (xun gu feng). The contents of aristolochic acid were determined by HPLC, the cumulative dosage correlating with the rapidity of progression within the chronic cases[8].
The carcinogenicity of Aristolochia
The statement that “carcinogenic properties of aristolochic acid could only be found in rodents” is another unbelievable misapprehension of facts. Insights from animal experiments had only been the starting point. 1981 drugs containing aristolochic acid were banned by the Deutsches Bundesgesundheitsamt (German Health-Agency), after a distinct carcinogenicity had been proven experimenting with rats[10].
The Belgian cases showed, more than 40 percent of patients with AN developed malignancies, especially urothelial carcinomas of the upper urinary tract, but also renal cell and bladder carcinomas[11-14]. A current study talks of stringent evidence of the involvement of aristolochic acid in a substantial percentage of renal cell carcinoma cases in Taiwan[15].
A substance’s property of forming DNA-adducts is considered strong evidence for its carcinogenicity. A group of Heidelberg scientists could detect DNA adducts of aristolochic acid, or its metabolite aristolactam in tissue samples of various groups of cancer patients having been treated with Aristolochia herbs. Chris Dhaenens reasons, that these findings had been questioned by another scientist[16]. But DNA-adducts were also verified in numerous cases of cancer associated with aristolochic acid, by other independent researchers from the USA, Croatia and Taiwan[15,17,18]. DNA-adducts could be reproduced in animal-experiments after administering aristolochic acid[19]. In fact, it could be demonstrated, that the mutations in the tumor tissue were frequently triggered in a specific part of a certain gene, the tumor-suppressor gene TP53, that is characteristic for aristolochic acid[17,20]. The mutation deactivates this gene and promotes the development of cancer.
Epidemiological studies in Taiwan
Between 1997 and 2003, up to a third of Taiwan’s population ingested potentially Aristolochia containing medicines[21]; likewise, its population has the highest incidence of end-stage renal disease worldwide. A screening of 199,843 patients, after eliminating confounding influential factors, showed a significantly increased risk of chronic renal disease after ingesting more than 30g mu tong or more than 60g guang fang ji [24].
Another Taiwanese study showed an increased risk of developing urothelial carcinoma in patients with end-stage renal disease, after having ingested mu tong corresponding with an estimated amount of more than 100mg aristolochic acid[25]. It is very rare in medicine that such clear evidence of a substance’s carcinogenic impact can be found, without being dependent on concluding the effect on humans from animal experiments.
Conclusion
For sure, it is annoying, that the Aristolochia problem actually dating from a far back time in Europe, is held against us at every incongruous opportunity. Alas, publications making light of the matter, like the one of Chris Dhaenens, possibly contribute to the adversaries’ justification for opposing Chinese Medicine. Nevertheless - the Aristolochia tragedy being, or rather having been, a disaster for Chinese Medicine, in this respect is a clear exception of the rule. Chinese herbal medicine, competently practiced and with medicines administered in conforming high quality, is a safe therapy. In fact, it has been shown, that patients with a chronic renal disease in Taiwan, who had been treated with Chinese medicines without Aristolochia, manifested a lesser mortality than those without this therapy[26].
Centrum für Therapiesicherheit in der Chinesischen Arzneitherapie (CTCA),
(Center for Safety of Chinese Herbal Medicine (CTCA)), Berlin
References:
1. Dhaenens C. Aristolochia: The malignant lie and the benign truth. J Register Chin Herbal Med 2013;10:39-41
2. Dhaenens C. Aristolochia - die bösartige Lüge und die gutartige Wahrheit. Naturheilpraxis 2016;69:65-8
3. Debelle FD, Vanherweghem JL and Nortier JL. Aristolochic acid nephropathy: a worldwide problem. Kidney Int 2008;74:158-69
4. De Broe ME. On a nephrotoxic and carcinogenic slimming regimen. Am J Kidney Dis 1999;33:1171-3
5. Wiebrecht A. Über die Aristolochia-Nephropathie. Dt Zschr Akupunktur 2000;43:187-97
6. Gökmen MR, Cosyns JP, Arlt VM, et al. The epidemiology, diagnosis, and management of aristolochic acid nephropathy: a narrative review. Ann Intern Med 2013;158:469-77
7. Pena JM, Borras M, Ramos J and Montoliu J. Rapidly progressive interstitial renal fibrosis due to a chronic intake of a herb (Aristolochia pistolochia) infusion. Nephrol Dial Transplant 1996;11:1359-60
8. Yang L, Su T, Li XM, et al. Aristolochic acid nephropathy: variation in presentation and prognosis. Nephrol Dial Transplant 2012;27:292-8
9. Chen W, Chen Y and Li A. [The clinical and pathological manifestations of aristolochic acid nephropathy--the report of 58 cases] (Chinese). Zhonghua Yixue Zazhi 2001; 81:1101-5
10. Hagemann U, Grase R, Thiele A, et al. Probleme der Arzneimittelsicherheit: Aristolochiasäure, Münchner Med Wschr 1982;124:611-2
11. Cosyns JP, Jadoul M, Squifflet J-P, et al. Urothelial lesions in Chinese-herb nephropathy. Am J Kidney Dis 1999;33:1011-7
12. Nortier JL, Martinez M-CM, Schmeiser HH, et al. Urothelial carcinoma associated with the use of a Chinese herb (Aristolochia fangchi). New Engl J Med 2000;342:1686-92
13. Zlotta AR, Roumeguere T, Kuk C, et al. Select screening in a specific high-risk population of patients suggests a stage migration toward detection of non-muscle-invasive bladder cancer. Eur Urol 2011;59:1026-31
14. Lemy A, Wissing KM, Rorive S, et al. Late onset of bladder urothelial carcinoma after kidney transplantation for end-stage aristolochic acid nephropathy: a case series with 15-year follow-up. Am J Kidney Dis 2008;51:471-7
15. Hoang ML, Chen CH, Chen PC, et al. Aristolochic acid in the etiology of renal cell carcinoma. Cancer Epidemiol Biomarkers Prev 2016;25:1600-8
16. Pfohl-Leszkowicz A. Ochratoxin A and aristolochic acid involvement in nephropathies and associated urothelial tract tumours. Arh Hig Rada Toksikol 2009;60:465-83
17. Chen CH, Dickman KG, Moriya M, et al. Aristolochic acid-associated urothelial cancer in Taiwan. Proc Natl Acad Sci U S A 2012;109:8241-6
18. Jelakovic B, Karanovic S, Vukovic-Lela I, et al. Aristolactam-DNA adducts are a biomarker of environmental exposure to aristolochic acid. Kidney Int 2012;81:559-67
19. Dong H, Suzuki N, Torres MC, et al. Quantitative determination of aristolochic acid-derived DNA adducts in rats using 32P-postlabeling/polyacrylamide gel electrophoresis analysis. Drug Metab Dispos 2006;34:1122-7
20. Chen CH, Dickman KG, Huang CY, et al. Aristolochic acid-induced upper tract urothelial carcinoma in Taiwan: clinical characteristics and outcomes. Int J Cancer 2013;133:14-20
21. Hsieh SC, Lin IH, Tseng WL, et al. Prescription profile of potentially aristolochic acid containing Chinese herbal products: an analysis of National Heath Insurance data in Taiwan between 1997 and 2003. BioMed Central 2008;3:1-6
22. Guh JY, Chen HC, Tsai JF and Chuang LY. Herbal therapy is associated with the risk of CKD in adults not using analgesics in Taiwan. Am J Kidney Dis 2007;49:626-33
23. Lai MN, Lai JN, Chen PC, et al. Increased risks of chronic kidney disease associated with prescribed Chinese herbal products suspected to contain aristolochic acid. Nephrology 2009;14:227-34
24. Lai MN, Wang SM, Chen PC, et al. Population-based case-control study of Chinese herbal products containing aristolochic acid and urinary tract cancer risk. J Natl Cancer Inst 2010;102:179-86
25. Wang SM, Lai MN, Wei A, et al. Increased risk of urinary tract cancer in ESRD patients associated with usage of Chinese herbal products suspected of containing aristolochic acid. PLoS One 2014;9:e105218
26. Hsieh CF, Huang SL, Chen CL, et al. Non-aristolochic acid prescribed Chinese herbal medicines and the risk of mortality in patients with chronic kidney disease: results from a population-based follow-up study. BMJ Open 2014;4:e004033